




Anatomy and ideal proportion :
A young face is defined by an overall “V” or inverted triangle shape given by full cheeks, prominent and high cheekbones with an upward and outward orientation of oblique shadow areas, associated with a well-defined facial oval.
Mechanism of facial aging:
Facial aging is due to sagging of the skin and stretching of the various structural ligaments, but also due to sagging of the musculoaponeurotic system (SMAS). The face sinks downwards with the appearance of nasolabial folds and jowls. This loss of elasticity leading to sagging skin is combined with a melting of the various fatty areas of the face over time, which leads to a loss of support.
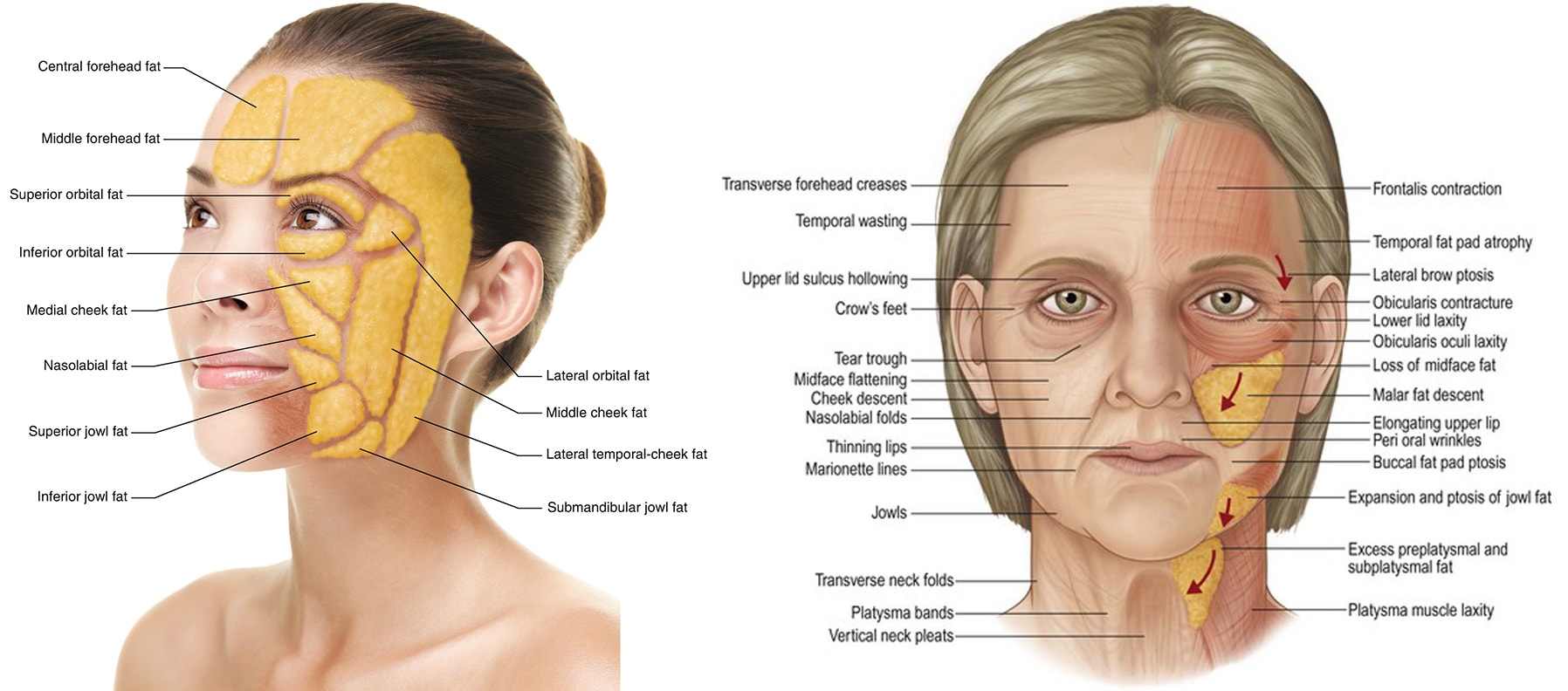
As a result, the cheek , temporal structures and eyebrow tend to descend downward. The malar fat pad, the eyebrow and temples can be surgically repositioned upward and laterally using an endoscopic technique (hidden incisions within the hairline, using a camera-assisted surgical approach).
Technique :
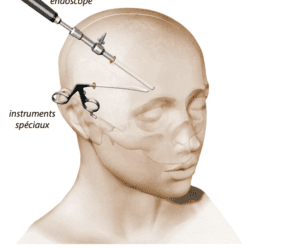
Hidden incisions are made in the scalp. A deep-plane dissection, in contact with the bone, is performed to release all attachments of the cheek, brow, and temple. These structures are then repositioned using oblique and vertical vectors and suspended using non-resorbable surgical sutures “cable sutures” anchored to the bone.
A canthopexy (repositioning of the lateral canthal ligament) may also be performed during the procedure to achieve a cat-eye effect.
Results:
Time frame final results:
Hypercorrection for 2 weeks, 3 weeks to see a significant result, 2 to 5 months to see the final result
Longevity of results :
5-10 years
Before surgery :
Smoking must be stopped 1 month before the operation (risk of skin necrosis is important if you smoke)
Do not take Aspirin 10 days before surgery, inform Dr. Lucas of any anticoagulant medication (Sintrom, Coumadin, Eliquis, etc..) to arrange for its discontinuation or replacement.
Take Arnica capsules 5 capsules 5 times a day for 5 days before surgery to prevent hematoma.
Intervention :
Pain: the pain after the intervention will be almost non-existent, with an adapted painkiller treatment
Duration of the procedure: 120-150 minutes
Anesthesia: sedation IV or general
Location: operating theater
After surgery:
Post-operative pain: 1/10
Social eviction : 2 weeks (hypercorrection, hematoma and swelling)
Resumption of work: 2 weeks
Resumption of sports: 3 weeks
Instructions:
Bed rest without major effort (which can cause the opening of small vessels during effort and lead to a hematoma) for 48 hours
Ice for 1 week, as often as possible, to reduce swelling
Arnica capsules 5 times a day for 5 days after surgery to prevent hematoma
Stop smoking permanently to prolong the effect and minimize complications
Surgery :
Control Dr Lucas D1, D2, D7, 3 weeks, 3 months, 6 months, 1 year
Removal of the threads at 7 days
Sun protection with an index greater than 50 for 6 months following surgery.
Follow-up of the scar by Dr. Lucas for 1 year after surgery is essential.
Complications
-Hematomas: they may require evacuation if they are large or too painful.
-Infection
-Asymmetry
-Ectropion (retraction of the lower eyelid) is possible in this type of surgery. This complication remains rare, but its proper management is necessary to prevent any risk of ocular complications (irritation, inflammation, dryness). A tendency to round eyes can also be observed.
-Nerve damage: in particular, paralysis of the temporal branch of the facial nerve responsible for raising the eyebrow. This results in an impossibility of raising the eyebrow with an asymmetry on both sides. This asymmetry is most often temporary and botulinum toxin injected into the other eyebrow makes it possible to obtain, if the patient so desires, symmetry during the recovery period. However, in some cases, it can be permanent.
– Loss of sensitivity of an upper hemi-lip is sometimes observed. It is most often reversible.